



In 2023, the Centers for Medicare & Medicaid Services (CMS) in the United States reported that more than 300 hospitals across 37 states had adopted Hospital-at-Home (HaH) programs under its Acute Hospital Care at Home initiative. Early data showed that these programs contributed to reduced readmission rates and lower healthcare costs, while maintaining comparable clinical outcomes to inpatient care.
Meanwhile in Singapore, the Ministry of Health (MOH) has actively expanded Hospital-at-Home models since 2020, with pilot programs demonstrating safe delivery of acute care at home, particularly for elderly and chronic disease patients. According to MOH-supported studies, these programs helped alleviate hospital bed shortages while maintaining quality of care through remote monitoring and structured clinical oversight.
At the same time, chronic diseases remain the leading burden on healthcare systems globally. The World Health Organization (WHO, 2023) estimates that chronic conditions such as cardiovascular disease, diabetes, and respiratory illnesses account for over 74% of global deaths annually. In both the U.S. and Singapore, these conditions are also among the most common reasons for hospitalization, emergency care, and long-term treatment.
These trends are reshaping how healthcare is delivered. Increasingly, providers are asking whether hospital-level care, especially for chronic disease management and early-stage intervention, can be delivered safely outside traditional facilities.
What is Hospital at Home?

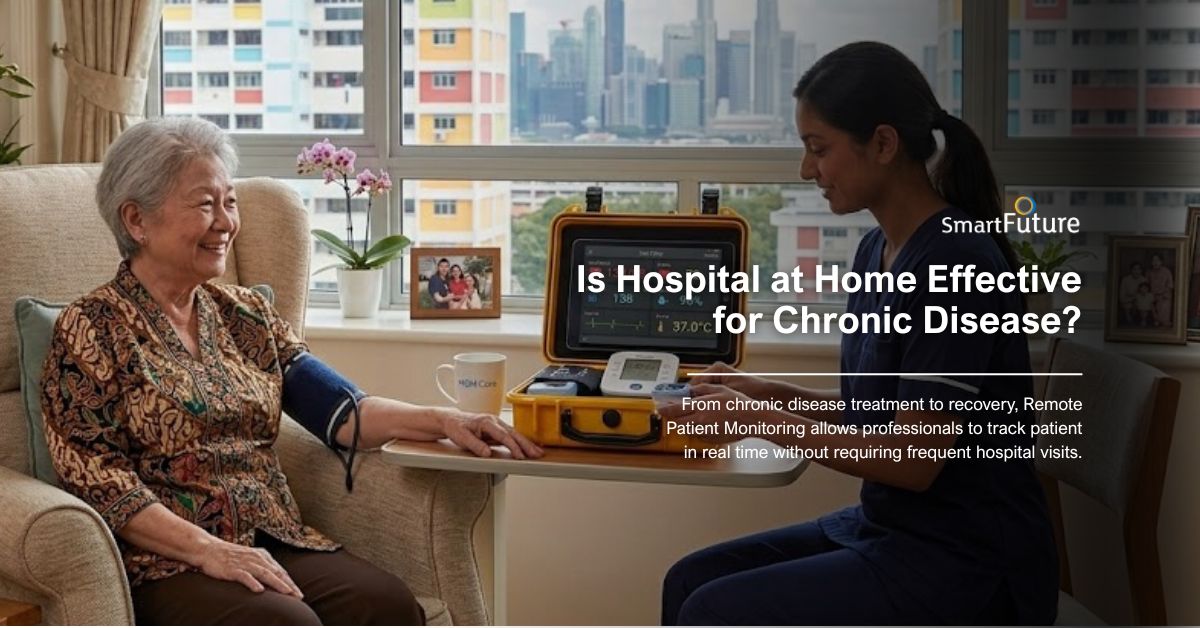
Hospital at Home is a care model that delivers hospital-level services directly in a patient’s home, replacing or shortening traditional inpatient stays.
Instead of being admitted to a hospital ward, eligible patients receive:
- Daily virtual consultations with physicians
- In-home nursing support
- Medication administration
- Continuous monitoring through connected medical devices
This model allows patients to recover in familiar environments while still receiving clinical-grade care.
In Singapore, Hospital-at-Home programs are being integrated into public healthcare systems to reduce strain on hospitals. In the U.S., major healthcare providers and insurers have expanded HaH programs as part of value-based care strategies.
Why Chronic Disease Needs a New Care Model
Chronic diseases such as diabetes, hypertension, COPD, and heart disease account for a significant portion of global healthcare utilization.
In the U.S., chronic diseases contribute to over 70% of healthcare spending, while in Singapore, they are among the leading causes of hospitalization and long-term care demand.
Traditional hospital-based care presents several challenges:
- Frequent readmissions
- High operational costs
- Limited bed capacity
- Patient discomfort and risk of hospital-acquired infections
By utilizing Hospital at Home, we are offered a solution by shifting care from reactive hospital visits to continuous, proactive management at home.
Chronic Diseases That Benefit from Hospital at Home
Diabetes
Patients with diabetes require continuous monitoring of glucose levels, blood pressure, and weight. Hospital-at-Home programs allow clinicians to track these metrics remotely and adjust treatment plans in real time.
Hypertension
Hypertension management relies heavily on consistent monitoring. With connected blood pressure devices, patients can be observed daily without needing frequent clinic visits.
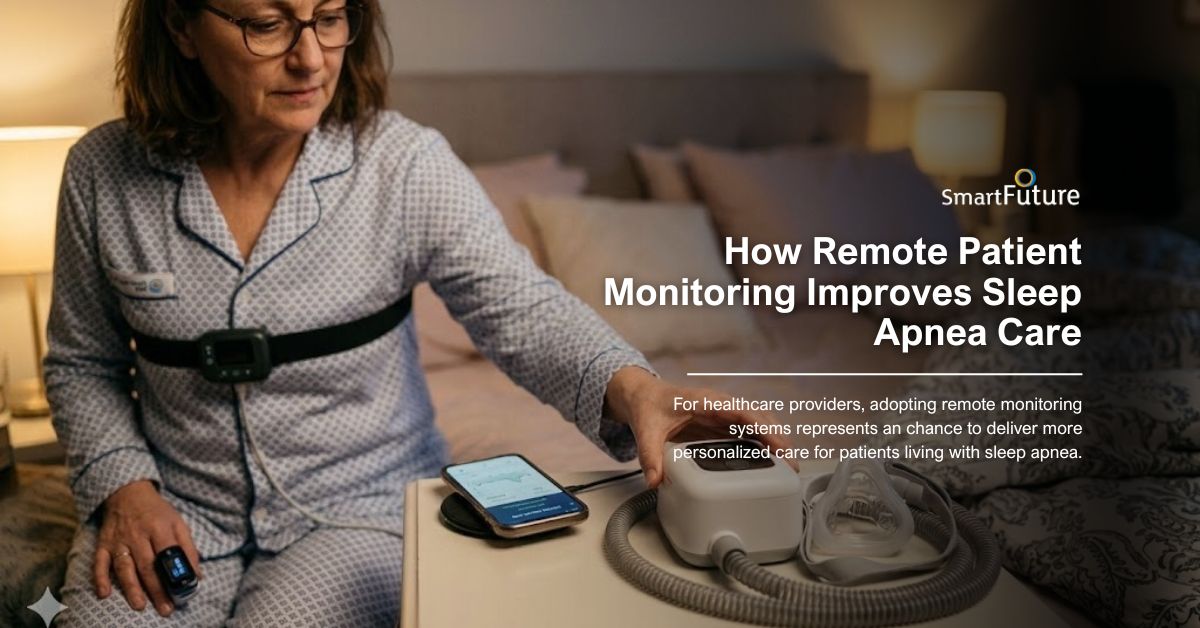
Chronic Obstructive Pulmonary Disease (COPD)
COPD patients are highly vulnerable to exacerbations. Monitoring oxygen saturation and respiratory patterns at home enables early intervention, reducing emergency hospital admissions.
Heart Disease
For patients with heart failure or cardiovascular conditions, tracking weight changes, oxygen levels, and heart function is critical. Hospital-at-Home programs help detect early signs of deterioration, such as fluid retention or abnormal vital signs.
Technologies Enabling Hospital at Home
The success of Hospital at Home depends on a combination of medical technology and digital connectivity.
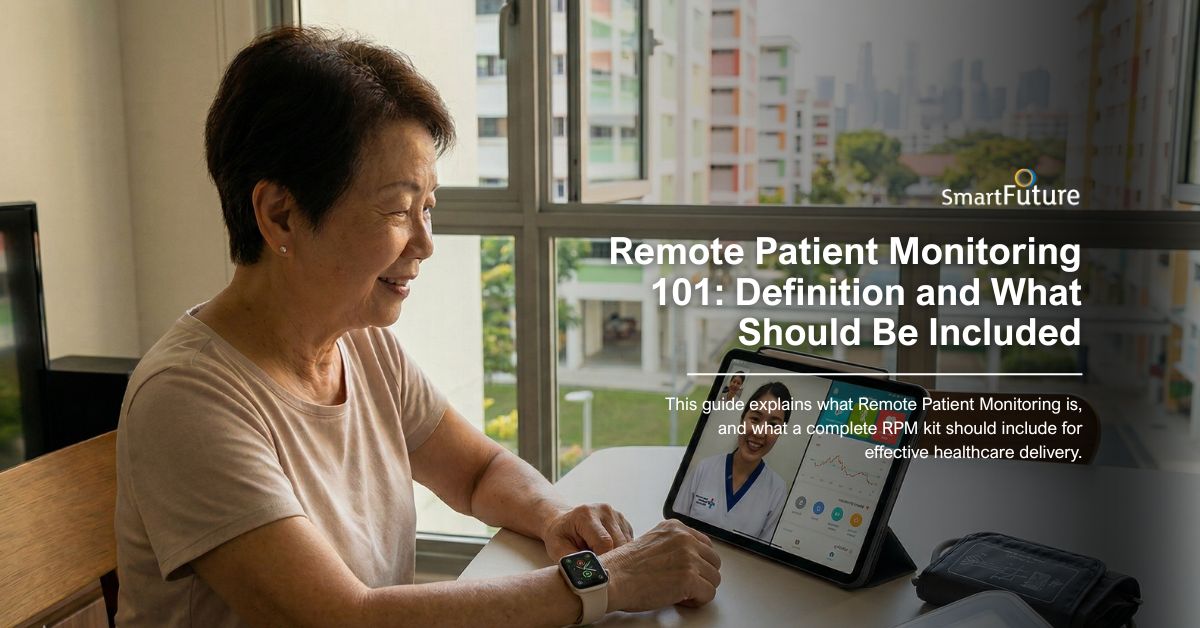
Remote Patient Monitoring Kits
These kits include medical-grade devices that track vital signs continuously. Data is transmitted to healthcare providers in real time, enabling proactive care.
Teleconsultation
Virtual consultations allow physicians to assess patients daily without requiring physical visits. This ensures continuity of care while reducing logistical barriers.
Portable Diagnostics
Portable medical equipment enables in-home testing, reducing the need for hospital-based diagnostics.
Together, these technologies create a connected care ecosystem that supports hospital-level treatment at home.
Clinical Benefits of Hospital at Home
Lower Healthcare Costs
Hospital-at-Home programs have demonstrated significant cost savings by reducing inpatient stays, minimizing emergency visits, and optimizing resource utilization.
Improved Patient Satisfaction
Patients consistently report higher satisfaction when treated at home. Familiar surroundings reduce stress, improve comfort, and support faster recovery.
Reduced Hospital Overcrowding
By shifting eligible patients out of hospital beds, healthcare systems can allocate resources to more critical cases. This is particularly important in urban environments like Singapore.
Reduced Risk of Hospital-Acquired Infections
Home-based care significantly lowers exposure to infections commonly associated with hospital stays.
The Role of Smart Future in Hospital at Home
As Hospital-at-Home models expand, the need for reliable, scalable monitoring solutions becomes critical. This is where Smart Future’s Direct Home Medical Kits play a key role.
Smart Future provides Hospital in Home solutions designed to support healthcare providers, clinics, and home care agencies in delivering hospital-grade care outside traditional settings.
What’s Included in Smart Future Kits
View this post on Instagram
Smart Future’s Direct Home Medical Kits typically include:
- Pulse Oximeter – for monitoring oxygen saturation
- Blood Pressure Monitor – for cardiovascular tracking
- Pulse Meter – for heart rate monitoring
- Weight Scale – for detecting fluid retention and metabolic changes
The device’s inclusion can be customized and is integrated into a centralized system that delivers:
- Real-time data tracking
- Customizable thresholds for alerts
- Automated health reports
- Secure dashboards for clinicians
This allows healthcare providers to monitor multiple patients simultaneously while maintaining high clinical standards.
Bridging the Gap Between Hospital and Home
The effectiveness of Hospital at Home for chronic disease management depends on one critical factor: continuous, accurate monitoring.
Without reliable data, home-based care risks becoming reactive rather than preventive. With integrated Remote Patient Monitoring and Direct Home Medical Kits, however, healthcare providers can deliver proactive, data-driven care.
Smart Future bridges this gap by enabling:
- Early detection of health deterioration
- Timely clinical interventions
- Scalable remote care programs
- Seamless integration into existing healthcare systems
- The Future of Chronic Disease Management
As healthcare systems in Singapore, the United States, and beyond continue to evolve, Hospital at Home is becoming a cornerstone of modern care delivery.
For chronic disease management, this model offers a sustainable solution that balances:
- Clinical effectiveness
- Cost efficiency
- Patient-centered care
With the support of advanced monitoring technologies and partners like Smart Future, Hospital at Home can quickly become the future standard of care.
For healthcare providers and organizations exploring this model, the question is no longer whether it works, but how quickly it can be implemented effectively.






 +65 8836 0984
+65 8836 0984 sales@oursmartfuture.com
sales@oursmartfuture.com 246 Macpherson Road, #03-01 Betime
246 Macpherson Road, #03-01 Betime 



